Lily is super happy. She loves life and dancing. Her smile is contagious!
Last fall, we thought she had a case of the flu. She went to see her doctor that day for an ear infection, but the doctor thought her coloring was off and sent her for blood work. She was diagnosed with Acute Myeloid Leukemia or AML. AML is a fast growing cancer of the bone marrow. We were given a 75% surivival rate. She needs to get a bone marrow transplant but has to wait because her heart function has went down a great deal.
Lily has been through so much at her young age. Her treatments have included bone marrow biopsies, spinal taps, chemotherapy, blood transfusions, and endless other tests. We can’t go many places when her blood counts are low.
A cancer diagnosis in our child has greatly affected our family life. We can’t be together that much and the kids miss each other. It is a difficult situation!
Childhood Leukemia. One of many words you don’t want to hear out of a doctor’s mouth, especially following, “Your child has.” About 5,400 families every year are swept up in the turmoil that is leukemia. While a diagnosis of leukemia is terrifying and tumultuous at best, the term “leukemia” is no longer the death sentence it once was. Just 60 years ago the survival rate for leukemia, the most common form of cancer in children, went from having a 3% survival rate to over a 92% survival rate.
It may surprise you to know that there isn’t just one pediatric leukemia. There are actually four types, with two of them being the most common: acute lymphocytic leukemia (ALL), which makes up about ¾ of the childhood cases of leukemia and acute myeloid leukemia (AML), which comprises nearly all of the other cases of childhood leukemia.
Children diagnosed with either of these today have a long, rough road ahead of them but a positive prognosis with an 80% five-year survival rate for ALL and 60%-70% five-year survival rate for AML.
Henry, diagnosed with ALL.
WHAT IS CHILDHOOD LEUKEMIA?
Leukemia is a cancer of the blood and bone marrow. Both ALL and AML begin when the bone marrow creates and accumulates too many immature blood cells. These extra cells turn into cancerous cells, replace the healthy cells, and are carried throughout the body in the bloodstream, causing the myriad symptoms leukemia often presents with.
Specifically in ALL, the cells that become cancerous are the cells that prevent germs from invading the bloodstream and tell the body’s immune system to kick in. These are called lymphocytes. In AML, the cells that become cancerous are the cells that destroy bacteria and digest diseased cells, called myeloid cells.
There are two other forms of leukemia: chronic lymphoblastic leukemia (CLL) and chronic myelogenous leukemia (CML). Just a glance at the names allows one to see the resemblance to their sister cancers, but unlike their acute counterparts, the term “chronic” means slowly progressing. While ALL and AML begin with immature cells, CLL and CML begin when the marrow produces too many mature cells. Fortunately, these chronic subtypes are very rare in childhood.
COMMON SYMPTOMS
Generally speaking, the symptoms of leukemia could be normal symptoms of many things far less scary than cancer. Just because a child presents with one or two of these does not mean they have cancer. A few of the following symptoms are the same symptoms as the common flu. That being said, these symptoms must be brought up to your pediatrician, especially if the flu-like symptoms have remained longer than a normal bout of the flu.
Leading up to Shephard’s ALL diagnosis, he had a swollen knee and fever that couldn’t be controlled with medication. He was also very lethargic.
ALL and AML share most symptoms. With ALL, the following symptoms are causes for concern:
Fever
Easy bruising and/or bleeding
Rash-looking pin point red dots called petechiae beneath the skin
Bone and/or joint pain
Lumps in neck, underarm, stomach or groin areas or lymph node locations
Discomfort, pain or feeling full beneath rib cage
Pale skin
Weakness
Lethargy
Loss of appetite
AML presents with some of the same symptoms:
Fever
Lethargy
Loss of appetite
And some different ones:
Night sweats
Weight loss
Ariana was constantly sick with several urgent care visits for over a month before her diagnosis. Her illnesses ranged from sinus issues, upper respiratory problems, ear infections and pneumonia.
All in all, when in doubt, a doctor visit is in order. These cancers are curable, but like their names imply, fast-moving.
Road to a Cure
With any illness, there is a trial and error period of medicines, tests and therapies before doctors finally get it right and have some amount of success; oftentimes, this trial and error period is continual, always searching for something better. Leukemia treatment is no exception. Trial and error was definitely the catalyst in finding the cure and continues today with research.
As recently as the early 1960s, leukemia patients always succumbed to their illness. ALWAYS. This is because of the fast growing rate of disease and infections related to the disease. Fast-forward less than half a century and we have an uplifting leukemia history lesson in 10 words or less: what was once a death sentence is now curable!
In the late 1940s doctors and specialists treated leukemia with a folic acid inhibitor, allowing patients a temporary remission. With this promise of some remission, the drug paved the path of chemotherapy for treatment of leukemia. Unfortunately, all patients eventually succumbed to the recurrence of their cancers.
By the 1950s, advances were being made with the combination therapy of corticosteroids and a drug called 6-MP, which was designed to kill rapidly growing cells like acute leukemic cells. This gave patients an improvement in quality of life while battling the disease and lengthened their life span, a promising outlook now on the horizon. Sadly, patients treated with this protocol still ended up dying from their disease as the leukemia developed a resistance to the drugs used to fight it and returned in other areas of the body.
In the 1960s, clinical trials focused on treating the recurrent cancers that fought off the treatments. Eventually, about half of the patients were cured of their cancers! By 1971, what was once deemed an impossibility became an amazing reality – doctors announced that leukemia could be cured. In 30 years of medical trials and scientific approaches, human beings cured cancer. A humbling experience that I can only imagine.
Since then, advancements have propelled the cure rate to 60% – sometimes greater than 90%. Some amazing advancements include cleaner and safer blood transfusions; refined chemotherapy protocols; bone marrow transplants from unrelated donors; and a special type of radiation called total body irradiation, a procedure to radiate the cancer cells in marrow pre-transplant, allowing the transplant better odds with a cleaner, less disease-ridden base of marrow.
The treatment of leukemia began in a time when blood was stored in glass milk bottles with paper cup caps and delivered to patients through a mesh-stuffed funnel. How far we’ve come in 70 years! These advancements are nothing short of medical miracles.
Treatment
Today, the standard treatment plan is similar for both types of acute leukemias. Most doctors place on their patients with ALL a three-stage process of treatment. For patients with the myeloid type (AML), normally only the first two stages are necessary.
Lucas’ treatment lasted 3 years and 3 months. He has been off treatment for 2 years and doing great!
Stage One: Remission Induction
The purpose of this stage is to kill the majority of the cancerous cells found in blood and/or bone marrow. This stage uses intense chemo protocols and most of the time requires long hospital stays. Because of the depletion of healthy cells also, this stage will usually require blood transfusions to infuse healthy blood cells back into the body. The majority of patients enter remission in this stage!
Stage Two: Consolidation
Another intense round of chemo kills any remaining cancer cells.
Stage Three: Maintenance/Continued Therapy
Kills the final remaining cancer cells and prevents relapse.
Bone marrow and stem cell transplants are offered if the leukemia doesn’t respond to standard treatment or comes back after remission. During a bone marrow transplant, bone marrow cells can be taken from the patient prior to treatment or from a donor in the hopes of creating a new “blood factory”, producing healthy white blood cells. Stem cell transplants are similar, introducing healthy blood stem cells to the patient for the same purpose. These stem cells can also come from the patient prior to treatment or from newborn cord blood donations.
Radiation therapy is offered if the cancer has spread to the brain or to the central nervous system or is likely to spread there. Strong radiation beams are aimed precisely at the target locations, killing the diseased cells.
TAKE ACTION
Any help offer to a family going through a child’s cancer diagnosis will always be appreciated, but there are two big ways to help give the biggest impact: blood donation and bone marrow donation.
Leukemia patients routinely need donated blood when they have low counts or they have a reduction of healthy blood cells. The American Red Cross blood drives are popular and easy ways to give blood. Giving blood is a very safe, relatively quick, and pretty painless procedure. Visiting the Red Cross website will give you all the facts you need before donating.
Bone marrow donation is a little more involved, but the good is does is by far more important! Joining the registry is easy! All it takes is a simple cheek swab. If donating bone marrow sounds like something you’d love to do for kids battling leukemia, visit the bone marrow registry at https://www.bethematch.org to learn more about saving lives with your generous donation.
If donating isn’t possible or you want to help even more, just giving your time to the family can make a huge difference for them. Offer a break during a lengthy hospital stay by sitting with their child while they get a much-needed reprieve from all things illness, send them a meal, make a care basket, or simply call. Find more ways to help here.
Hope
Let me leave you with a uplifting story of a child fighting the fight of her life against leukemia and winning, thanks to a selfless gift from a stranger:
“Olivia was 19 months old when she was diagnosed with very high risk T-Cell ALL. Her disease did not respond to standard treatment and it was determined that she would require a bone marrow transplant in order to have any hope for survival. Thanks to an anonymous donor, she received her second chance at life, just a few days after her second birthday. She has now been in remission for over three years and has been living a very normal and happy life. We were lucky enough to be able to meet her wonderful donor this past December and thank him personally. Although Olivia will be followed by a rather large team of medical specialists for the rest of her life, we are beyond grateful that she is still here with us today. We are also very thankful for organizations like The Gold Hope Project, that help us to document her life. These are truly priceless gifts for our family.”
Olivia, ALL survivor.
Thanks to medical advances, big-hearted blood and marrow donors and generous donations to children’s cancer research, leukemia is still a dirty word, but now one capable of being washed away.
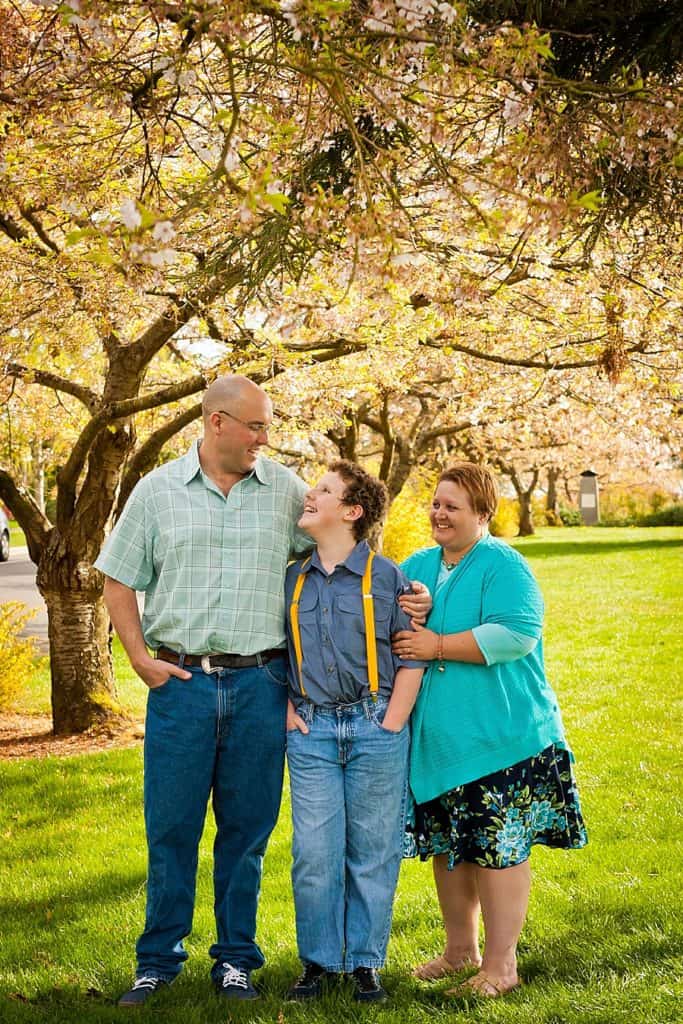
Torin is all about everything geek (Dungeons and Dragons, Dr Who, wizardry, Star Wars, etc. He loves computer games and volunteers with a little boy who has a neuromuscular disorder to teach him Minecraft. He loves reading joke books and being silly. He is an amateur novelist and is working on his third novel.
Torin had some issues with balance, coordination and energy level but we had no idea cancer was the cause was until Feb of 2009 when he became very sick with hydrocephalus. His MRI showed enhancement but no mass. He was in a lot of pain and vomitted continually. He had an external shunt placed and was hospitalized for 12 days. He had a lot of testing. There were cancer cells found in his spinal fluid but they scanned his whole body without finding a mass. The external shunt was removed and we were released but had to go back after 36 hours because the hydrocephalus had not resolved and he was very ill. He got his VP shunt at that point. We went on watch and wait and his tumur progressed to the point they could safely perform a biopsy. Torin was diagnosed with a high risk malignant brain tumor on 9/9/09 after six months of symptoms. His diagnosis is diffuse leptomeningeal PNET.
PNETs usually occur in the cerebrum and have a tendency to spread. Like many tumors, the exact cause is unknown. Standard treatment usually includes surgery but total removal of the tumor, due to many varying factors, is usually near impossible. PNETs usually occur in young children.
Torin had a very high dose of radiation because there was no tumor bed to boost. He also had high dose chemotherapy.
Since Torin’s diagnosis, we have clarified our priorities and make the most of our time. We are still sorting out some of the ways the trauma during treatment has affected our family relationships. We have come a long way together.
Henrik…oh what a card! Henrik just turned twelve years old. He is such a compassionate young man, and so so funny! He loves to tell jokes (especially blonde jokes). He has taught himself how to beat box, loves music, comedies, animals, nature, and science. Henrik is really special – I know all kids are- but he’s an old soul. He’s so smart. He’s been in advanced classes at school since 3rd grade.
Henrik was having headaches, spots in his vision and general fatigue when he was diagnosed with mixed cell pineal region germ cell tumor (a brain tumor) on May 2, 2014. Henrik has now had three brain surgeries, chemotherapy, and radiation. He has a mixed cell tumor, and one type will not respond to treatment (and is inoperable). He will be getting MRI’s every 3 months for a few years, and eventually at least one a year for life. He may be facing surgery again at some point. It’s caused so many emotional struggles, as well as financial for our family. Between unpaid FMLA (Henrik’s dad) and his mom staying at home to care for him, bills have piled up.
Henrik has had to either be in the hospital or at home for a lot of the past 19 months. He’s still in school but it’s become a bit of a struggle at times for him to catch up. Since the tumor, he’s had to go to mainstream math due to some issues with learning. He isn’t able to play sports so is not in PE at school, so instead he is a teacher’s aid for one period. He tutors a boy who needs special help with reading and LOVES doing it!
His mother no longer works outside of the home so that she can tend to his medical and emotional needs. Henrik cancer diagnosis has brought their family together spiritually and emotionally.
Today the photographer spotlight is on Jessica Mielke (Photo Art by Jessica). Jessica is a maternity, birth and documentary family photographer located in Aurora Colorado. She has two crazy kids and amazing husband who serves in the United States Air Force. As a family they enjoy hiking, baking and traveling. She has been a photographer for five years now and couldn’t imagine doing anything else. Jessica really loves volunteering for The Gold Hope Project and hopes to help spread the word about how this organization can benefit childhood cancer patients and their families.
What made you want to join tghp as a volunteer?
I wanted to become a gold hope project volunteer for a while and a friend of mine has a son with re-diagnosed Langerhans Cell Histiocytosis (LCH) While I provided photography services for them, I felt compelled to volunteer my services further. Knowing how much those images will be cherished by that family forever pushed me into becoming a volunteer.
What is your favorite thing about being a Gold Hope Project photographer?
I have only done a few sessions with The Gold Hope Project but seeing how strong those families and children are is really, truly inspiring.
Has working with children with cancer changed anything in your life?
It has really made us slow down and put the meaningless stuff behind us. We don’t bicker as much and we are trying to build more long lasting memories with our children. I also make it a point to photograph my kids every single day.
What is one thing you hope to families you photograph for the project can take away from this experience?
That no matter what your life situation might look like right now, life is beautiful and it is a gift. I really hope that the families and children I have photographed feel beautiful.
How would you describe your photography?
I am a documentary and lifestyle photographer. My goal is to provide my clients with beautiful real life images.
Where are you located?
I recently relocated to the Aurora Colorado and I am photographing in the Greater Denver Metro area.